Pediatric penetrating oropharyngeal trauma
- 738Downloads
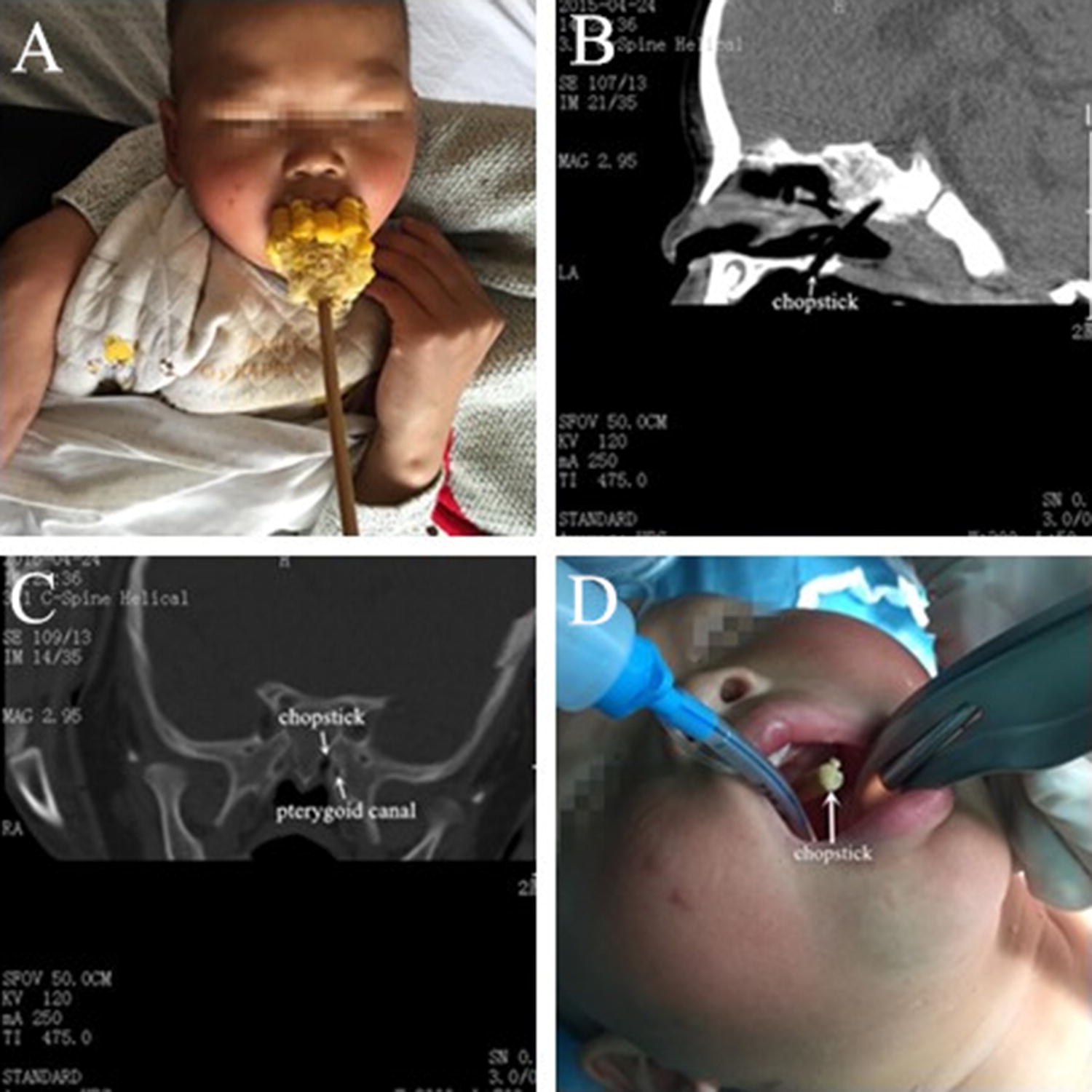
Anesthesia management of a pediatric patient with penetrating oropharyngeal trauma. A) A cobcorn skewered by a chopstick occluded the mouth. B) A sagittal computed tomography (CT) scan showed that the chopstick had lodged in the skull base, with the coronal CT image (C) showing that the chopstick had passed through the inner edge of the medial plate of the pterygoid canal. D) The patient was successfully intubated after the corncob had been removed and the chopstick cut away to allow laryngoscopy.
This case presented the anesthetic dilemma of mananging a full stomach and near complete obstruction of the oral airway. It is important to consider that the patient would likely have aspirated had he vomited, even though he was alert and had intact protective airway reflexes when he presented, as the nasal airway was too small to remove stomach contents. Also, as the penetrating oropharyngeal trauma may have caused major vascular injuries as a lateral soft palate or peritonsillar injury could have posed a potential risk to the internal carotid artery injury,1 a CT scan was urgently conducted. Had a vascular injury been suspected, CT angiography could have further identified its extent.2 Based on this patient's CT scan, if he had started to vomit before commencing surgery, we would have immediately removed the chopstick and corncob to protect the airway, despite the potential risk of hemorrhage.
Notes
Acknowledgement
We are grateful to Guoming Xie MD, PhD, MSc who provided feedback on this paper.
Financial disclosure
This manuscript was supported by the Natural Science Foundation of Zhejiang Province Y17C09009).
Editorial responsibility
This submission was handled by Dr. Hilary P. Grocott, Editor-in-Chief, Canadian Journal of Anesthesia.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Soose RJ, Simons JP, Mandell DL. Evaluation and management of pediatric oropharyngeal trauma. Arch Otolaryngol Head Neck Surg 2006; 132: 446-51.CrossRefGoogle Scholar
- 2.Brietzke SE, Jones DT. Pediatric oropharyngeal trauma: what is the role of CT scan? Int J Pediatr Otorhinolaryngol 2005; 69: 669-79.CrossRefGoogle Scholar
Copyright information
Open AccessThis article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
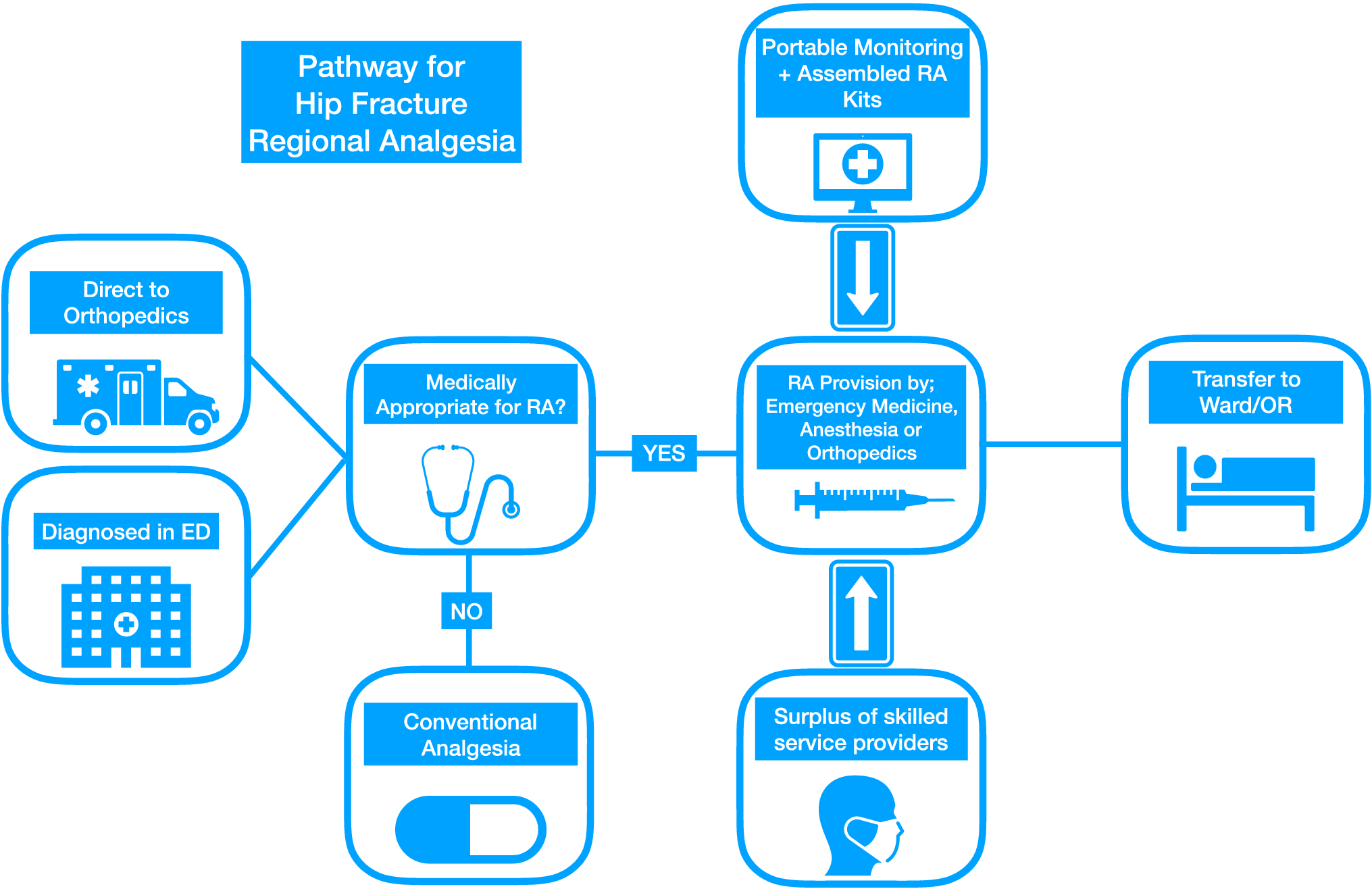
Improving care for elderly patients with hip fracture: interdisciplinary collaboration in regional analgesia
Anapafseos 5 . Agios Nikolaos
Crete.Greece.72100
2841026182
Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου
Σημείωση: Μόνο ένα μέλος αυτού του ιστολογίου μπορεί να αναρτήσει σχόλιο.